The Forensic Nurse
CRITICAL TESTING
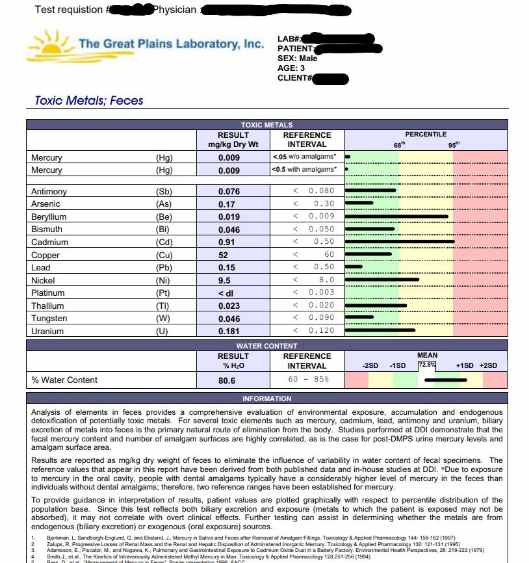
CADMIUM High Fecal CD
This test result is from a 3 year old male vaccine injured and metal toxic child. Approximately 90% of ingested Cd (Cadmium) is excreted through the feces and therefore fecal measurements of Cd can be used to estimate Cd ingestion and uptake. Cd adversely affects the kidneys, lungs, testes, arterial walls, and bones and interferes with many enzymatic reactions.
Chronic Cd excess (T 1/2 ~ 30 years) can lead to microcytic, hypochromic anemia and proteinuria with loss of beta-2-microglobin, and functional zinc deficiency. A recently published epidemiological study found a significant correlation between elevated hair Cd and distractibility in young children (Le Clair, J.A. and D.W. Quig. Mineral Status, Toxic Metal Exposure and Children's Behavior. J. Orthomol. Med. (2001) 16: 13-32).
Cd excess is also commonly associated with fatigue, weight loss, osteomalacia, and lumbar pain. Cd absorption is reduced by zinc, calcium, and selenium. Cd is found in varying amounts in foods, from .04 ppm for some fruits to 3-5 ppm in some oysters and anchovies. Cigarette smoking significantly increases Cd intake. Refined carbohydrates have very little zinc in relation to the Cd.
Other sources of Cd include human biosolids, pigments and paints, batteries (Ni-Cd), plastics and synthetic rubber (tires). A confirming test for elevated body burden of Cd is urine analysis following administration of appropriate chelating agents: EDTA, sulfhydryl agents (DMSA,D-penicillamine, DMPS). Urinary beta-2-microglobulin is considered to be the best test for assessment of Cd-associated functional damage to the proximal tubules of the kidney.